Great tales start with, Once upon a time…
Great tales start with, Once upon a time…
Academics tell the story of Medicare like this:
Once upon a time, in the dark days before universal healthcare, patients lay at home suffering in pain. Wealthy patients went to shining hospitals with all the modern specialists they needed.
Everyone else traded potatoes and chickens for medicine offered by the rare doctor who would stoop to see them.
Patients died in pain. Or they sold their farms to pay for treatment, declared bankruptcy, and then died in pain from curable diseases.
In these dark days of pre-civilized Canada, one person started to campaign for the poor and oppressed. From the wilderness of Saskatchewan, someone finally stood up for patients.
When no one else cared, Tommy Douglas, champion of the poor and oppressed, dared to challenge the medical establishment. Mr. Douglas single-handedly attacked organized medicine.
He shamed doctors’ selfishness.
He demanded Canadians do what was right: provide free care for all, without consideration for patients’ ability to pay.
Mr. Douglas demanded that doctors put aside their greed for the sake of their patients. He forced doctors to put patients before income.
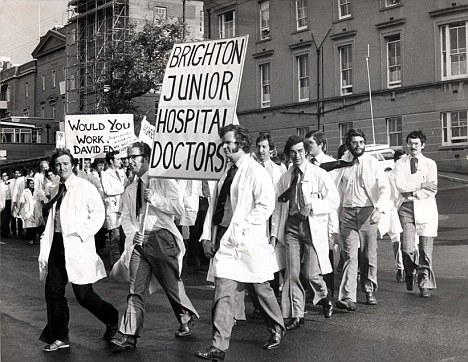
Doctors fought back. They went to war with Tommy Douglas and refused to see patients.
After a 23-day strike, doctors surrendered. They lost the war and submitted to Douglas’ plan of care for all, not just the rich and well connected.
Tommy Douglas gave Canadians Medicare.
Finally, no one would ever lose their farm to pay for medical bills. Now, people could take out business loans and invest in the economy. Mr. Douglas civilized medical care in Canada.
It was the dawn of a new age.
Doctors Vilified (Again)
But just when people started to celebrate, the doctors took a dying stab at Douglas’ dream. Doctors said they would agree to Medicare only if they could work ‘fee for service’ (FFS).
FFS was the condition of their truce.
Mr. Douglas desperately wanted to help the poor. So he compromised at the last minute. He gave doctors what they wanted: to be paid for each service they provided.
Poor Tommy did not know what he allowed. He let the fee-for-service virus infect Medicare.
Evil Fee for Service
Fee for service (FFS) paid doctors for services they performed. FFS drove doctors to invent procedures and to dream up new services to provide patients, whether patients needed them or not.
FFS drove up the cost of care.
It created run-away spending.
Doctors, ravenous for more and more income, worked and worked and worked. They toiled around the clock just to make more money, to bill more services.
Patients have suffered ever since.
Finally, the government said, Enough! FFS must go. We will put doctors on capitation.
And the golden age of primary care reform began. Now doctors work in teams, where patients get only as much care as they need.
And everyone lived happily ever after.
Reality
Theatrics aside, most people see doctors and government as reluctant partners for the last 40 years in Canada.
Every schoolboy knows that doctors have caused the situation we now find ourselves in: provinces unable to pay for care, and patients dying on wait lists.
In reality, before Tommy Douglas rescued Canada from doctors, there were insurance companies that covered the costs of acute care. Patients who could not afford to pay the premiums had the premiums covered by the government (see Setting the Record Straight: A Doctor’s Memoir Of The 1962 Medicare Crisis ).
).
The few people who refused insurance, and still could not afford care, saw doctors for free. Doctors believed their professional duty demanded that they treat people who could not pay. Either way, patients had coverage, if they wanted it.
Governments could choose to cover the insurance premiums for the poor. The option existed. If government did not, it was not for lack of ability to do so.
Greed vs. Freedom
Doctors’ incomes were not at stake in the strike in 1962. Doctors actually enjoyed a huge boost in pay under Medicare.
Finally, all their bills were paid. They could stop charity work and spend more time on things that paid.
Purely selfish motives should have led doctors to support Medicare from the start.
But they did not.
Tommy Douglas campaigned on a government takeover of healthcare. Doctors resisted government takeover on the belief that government cannot care for patients. Many doctors had fled the UK after seeing what government does, when they take command and control a whole industry.
Politicians, who control healthcare, end up treating it as a bauble to win support. They throw handouts to win votes; care to win elections.
Governments meddle and ration.
Politicians fund popular procedures, like sex reassignment surgery, and leave patients who need less popular treatment, like cancer care, to die on wait lists.
Politics
Tommy Douglas wanted to nationalize an industry because it fit with his political convictions.
He believed government could do a better job than anything designed by the citizens themselves. He believed a group of highly trained, super-smart elites, who worked for government, could serve patients better than a patchwork of doctors in communities across Canada.
Douglas passionately believed in the state – the government – as the most trusted force for good in society. He saw bureaucrats and politicians disinterestedly working for the ‘public good’ as the best way to provide care.
He fundamentally disagreed with Adam Smith, in The Wealth of Nations : businessmen do not try to serve their customers; they try to exploit customers at every turn.
: businessmen do not try to serve their customers; they try to exploit customers at every turn.
Wringing Our Hands Over Access
Today, we hear about desperate attempts for patients to see doctors on evenings and weekends.
Why won’t doctors see patients outside of office hours?
How selfish and insensitive!
No one in academia dares to tell the truth about this. Research grants and university tenure depend on government support for their institution.
The truth is this:
Government fixes the price for services as low as possible. It pays $33 for diagnosing pneumonia during the daytime, and a couple dollars more to see the same patient in the evening.
After paying a pittance for evening work, government castigates physicians for not providing access to patients in the evenings and on weekends.
Academics never mention this. They just wring their hands about how doctors do not seem to care about seeing patients after hours.
Doctors would LOVE to see their patients in the evenings! But billings must cover the cost of hiring staff willing to work after hours, or doctors work for free.
Government knows that if they pay an appropriate premium for doctors to work after-hours, and on weekends, like patients want, then doctors will provide ALL their services after-hours.
Doctors want to provide services that patients need, in a way that patients want them delivered.
But costs go up when doctors work to serve patients. Utilization, the amount of medical services delivered, increases.
So instead, government rations care by refusing to cover the cost of after-hours care and blames doctors for the lack of access.
Doctors Need to Speak Up
In a time of universal deceit, telling the truth is a revolutionary act.
G. Orwell
Doctors need to speak truth to power. They need to write, speak, publish, and do whatever they can to peacefully protest. Patients need to know.
Government has failed to deliver on its promise to provide care.
Canadians are under-insured.
Government took over a whole industry and then blames underperformance on doctors. Enough is enough.
When will people stop telling fairytales to feed political agendas?
Photo Credit: Encylopedia of Saskatchewan