 Clinicians and bureaucrats wrestle for control with talk of quality and accountability. Both sides crave concrete definitions. Accountability zealots want control of provider’s performance as if chaos would reign without policing.
Clinicians and bureaucrats wrestle for control with talk of quality and accountability. Both sides crave concrete definitions. Accountability zealots want control of provider’s performance as if chaos would reign without policing.
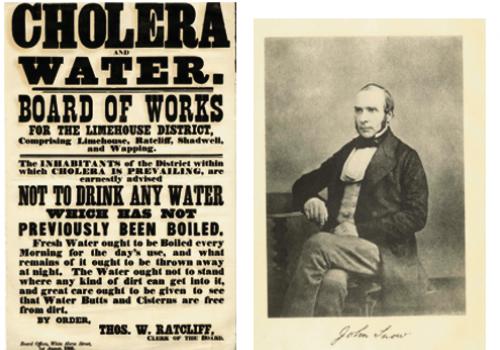
Healthcare delivery gets shaped using concrete metrics like HbA1c levels, blood pressure readings, or surgical complication rates.
People start to see medicine as nothing-but fixing high blood pressure, or normalizing sugar levels, or replacing hips.
But, if medicine is nothing-but controlling blood pressure or HbA1c, then it’s a product to be managed like any other.
If medicine is nothing-but matching patients with evidence, then quants can match populations with resources without input from physicians or nurses.
If we reduce medicine to technical outcomes, bureaucrats regulate with impunity.
Medicine is more than applied physiology.
Medicine applies science, but it is much more than applied science.
“[Medicine] is the totality of this unique combination which constitutes the clinical moment and the clinical encounter, without which authentic medicine does not exist. No simplistic neo-Cartesian reduction of medicine to sciences of mind, arithmetically added to science of the body and tied together with a ribbon of moral science, is adequate to explain this synthesis. Nor is this merely biology. Neither plants nor animals – granted they become ill as well as humans – can enter into a relationship with the healer in which the patient participates as subject and object simultaneously.” A Philosophical Basis of Medical Practice, Pellegrino and Thomasma.
Sure, we must improve clinical metrics. But, meaningful outcomes for patients are often qualitative, subjective, or impossible to measure. How do we measure surgical judgment beyond complication rates? How do we measure communication skills? Reasoning ability? Aptitude at interpreting non-verbal cues?
We need to learn how to articulate what medicine is. And, it must be hard. It needs to be tough and complicated to capture everything we do for patients. Narrow-minded medicine makes patients secondary.
We need a definition of medicine that starts with the clinical encounter and puts patients’ interests at the centre.