
 Television host, Steve Paikin, spoke with Dr. Ved Tandan, Ontario Medical Association President, about the failed OMA MOH negotiations. Paikin asked what happens when government, the payor, makes unilateral cuts.
Television host, Steve Paikin, spoke with Dr. Ved Tandan, Ontario Medical Association President, about the failed OMA MOH negotiations. Paikin asked what happens when government, the payor, makes unilateral cuts.
“Usually when these kinds of things break down, Dr. Tandan, the payee does something like withdraw services; like go to Queen’s Park with lab coats and protest signs and raise hell, etc., etc. What do the doctors have planned now?“
Tandan said, “The doctors of Ontario are going to do everything we can to minimize the impacts of these cuts. But make no mistake; there will be negative impacts.“
See The Agenda (11:38).
What Next?
A prominent pollster in Ontario told a large group of physicians that doctors need to learn how to play tough. They shouldn’t be so nice.
Ineffective action could be seen as inaction.
Physicians need to think about doctors who are working now, those who will follow, and all their patients. If doctors frame fee cuts as nothing but a personal nuisance, they miss the point. Current cuts drain physician funding for the next 15 years or more.
Time to Recovery
In 2012, doctors took a 5% fee cut. Inflation runs between 1.2-2% per year. The Wynne Liberals sliced off 2.65% this month with more to follow. Wynne promises 4% plus an unknown amount of claw backs as ‘reconciliation’ for growth in services.
5% + (2% x 2 years) +4% = 13%
Doctors will see 17% cuts, or more, to gross billings by 2017 including inflation. Physicians’ net income will drop well over 20%.
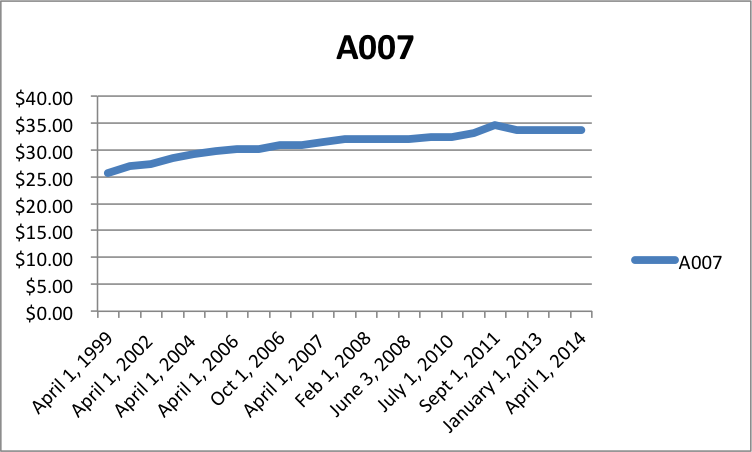 How long will it take to fees to recover? Even if we assume a 1% recovery per year, plus 2% inflation, it would take 17 years to recover with 3% raises per year, or 2034. How reasonable is it to expect 17 yrs of 3% raises? The core family practice code, A007, has almost flatlined.
How long will it take to fees to recover? Even if we assume a 1% recovery per year, plus 2% inflation, it would take 17 years to recover with 3% raises per year, or 2034. How reasonable is it to expect 17 yrs of 3% raises? The core family practice code, A007, has almost flatlined.
Response vs. Vision
Doctors took a fairly measured, coordinated response so far. Articles, videos, social media and meetings with politicians offer peaceful protest. Should physicians ramp up their response? Should they march to Queen’s Park?
What do doctors want? They probably want the bottomless pit of reconciliation abolished. Docs likely want the indiscriminate program and fee cuts reversed. But do physicians have a vision for fundamental change?
Without system change, we can expect more cuts and tweaks in the future. Political pilot projects within the current framework will raise expectations and then disappoint with unsustainable costs. Four decades make it certain. Dr. Max Gammon, after studying the British National Health Service, said that in
“a bureaucratic system … increase in expenditure will be matched by fall in production ….”
It’s called Gammon’s Law, or the Theory of Bureaucratic Displacement.
Some doctors want protest but have little appetite for fundamental change. Protesting current cuts while asking for a return to the status quo prolongs the inevitable. If we protest, we need protest with vision. Are doctors willing to consider substantive system change? Is the public ready for it?
Or should doctors shut up and accept a >20% cut to net income?
photo credit: theagenda.tvo.org

