
 Television host, Steve Paikin, spoke with Dr. Ved Tandan, Ontario Medical Association President, about the failed OMA MOH negotiations. Paikin asked what happens when government, the payor, makes unilateral cuts.
Television host, Steve Paikin, spoke with Dr. Ved Tandan, Ontario Medical Association President, about the failed OMA MOH negotiations. Paikin asked what happens when government, the payor, makes unilateral cuts.
“Usually when these kinds of things break down, Dr. Tandan, the payee does something like withdraw services; like go to Queen’s Park with lab coats and protest signs and raise hell, etc., etc. What do the doctors have planned now?“
Tandan said, “The doctors of Ontario are going to do everything we can to minimize the impacts of these cuts. But make no mistake; there will be negative impacts.“
See The Agenda (11:38).
What Next?
A prominent pollster in Ontario told a large group of physicians that doctors need to learn how to play tough. They shouldn’t be so nice.
Ineffective action could be seen as inaction.
Physicians need to think about doctors who are working now, those who will follow, and all their patients. If doctors frame fee cuts as nothing but a personal nuisance, they miss the point. Current cuts drain physician funding for the next 15 years or more.
Time to Recovery
In 2012, doctors took a 5% fee cut. Inflation runs between 1.2-2% per year. The Wynne Liberals sliced off 2.65% this month with more to follow. Wynne promises 4% plus an unknown amount of claw backs as ‘reconciliation’ for growth in services.
5% + (2% x 2 years) +4% = 13%
Doctors will see 17% cuts, or more, to gross billings by 2017 including inflation. Physicians’ net income will drop well over 20%.
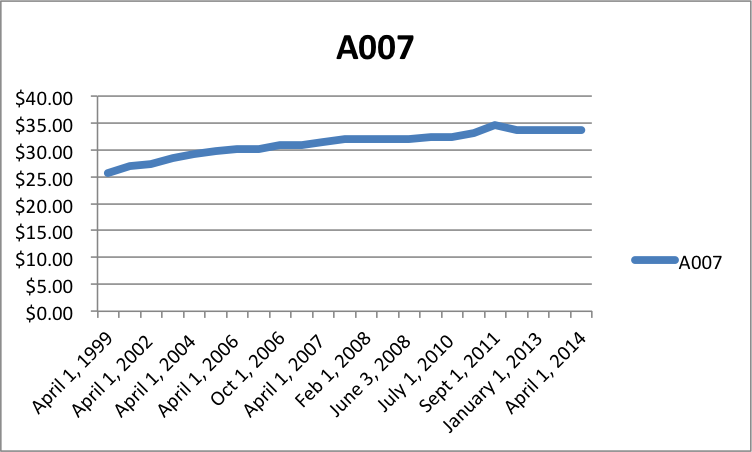 How long will it take to fees to recover? Even if we assume a 1% recovery per year, plus 2% inflation, it would take 17 years to recover with 3% raises per year, or 2034. How reasonable is it to expect 17 yrs of 3% raises? The core family practice code, A007, has almost flatlined.
How long will it take to fees to recover? Even if we assume a 1% recovery per year, plus 2% inflation, it would take 17 years to recover with 3% raises per year, or 2034. How reasonable is it to expect 17 yrs of 3% raises? The core family practice code, A007, has almost flatlined.
Response vs. Vision
Doctors took a fairly measured, coordinated response so far. Articles, videos, social media and meetings with politicians offer peaceful protest. Should physicians ramp up their response? Should they march to Queen’s Park?
What do doctors want? They probably want the bottomless pit of reconciliation abolished. Docs likely want the indiscriminate program and fee cuts reversed. But do physicians have a vision for fundamental change?
Without system change, we can expect more cuts and tweaks in the future. Political pilot projects within the current framework will raise expectations and then disappoint with unsustainable costs. Four decades make it certain. Dr. Max Gammon, after studying the British National Health Service, said that in
“a bureaucratic system … increase in expenditure will be matched by fall in production ….”
It’s called Gammon’s Law, or the Theory of Bureaucratic Displacement.
Some doctors want protest but have little appetite for fundamental change. Protesting current cuts while asking for a return to the status quo prolongs the inevitable. If we protest, we need protest with vision. Are doctors willing to consider substantive system change? Is the public ready for it?
Or should doctors shut up and accept a >20% cut to net income?
photo credit: theagenda.tvo.org
Shawn…accepting the 20% cut sets the tone for further cuts down the road. This sets you up for further humiliation and we the patients, longer waitlines and poor service from our HC providers.Everything about these negotiations are wrong. There are far too many changes required to ensure HC is solvent and effective for the long term. Govt must be persuaded to engaged with docs and then public. Doc Fullerton and yourself along with others that have considered solutions can make a difference for govt seeking to contain costs and a public that needs greater access and consistent care.
Bottom line, fight any cuts until govt comes to table willing to explore real change for the future.
Thank again for reading and sharing your thoughts, Don!
You nailed it with, “There are far too many changes required to ensure HC is solvent and effective for the long term.”
I think your advice is bang on. We need enough people alert to the issues to push for meaningful solutions.
Be well!
Shawn
The current imposition which is unacceptable,indicates to me that government has reached the stage where they feel that the provincial budget can no longer afford the increasing bill of Medicare.Faced with this situation,they will do whatever they can get away with to limit expenditures,including cutting back on the incomes of all service providers,rather than do the politically unpopular of looking at other means of funding.These other means do not automatically mean going to a two tier system,as they-could involve a return to health care premiums,increases in the health tax,and other income generating tax changes,all of which would be a political liability.At present their move to limit physicians incomes probably appears the best political option,and it will depend on the legal and care fall out from this .whether they will be forced to look at the other options.How we as a profession respond will have a definite effect on how this plays out,but passive acceptance by doctors and the OMA certainly is not an option.
Well said!
“…passive acceptance by doctors and the OMA certainly is not an option.” I agree.
If politicians refuse to discuss options beyond cutting doctors’ fees, then we should present options for debate. We cannot allow more of the same. I’ve been wondering whether doctors feel paralyzed by fear; fear that any system change might be far worse than what we have now. I also wonder whether those with passion to fight and vision for change have left the province over the last few decades. What will it take to awaken the bear; when will doctors fight back?
Thanks so much for reading and sharing your thoughts!
Best
Shawn
The discussion today is distinctly different than it was in the last major cut back,under Bob Rae.In that time the major topic was whether government monopoly of the method of doctor payment was either financially viable or acceptable for a professional service.Obviously those of us who doubted the latter did not win the debate,and we have had essentially 20 plus years of government only payment for medical services.During that period doctors were overall paid adequately,with some times of tension a reflection of economic hard times.
We are now into an era of economic tough times,worse than most in the past,and it remains to be seen if the profession will be as accepting of the government monopoly as a sole method of payment for necessary services.There are other options,if we have the will to demand that they be examined as an option,and assert, our status as true professionals.
Thanks again for sharing this, Bill.
You mention 20 plus years. Can you help me with this; didn’t it become illegal to bill outside of OHIP in 1984 with the Canada Health Act? I started medical school in 1992, so I didn’t pay attention to medical politics then.
I think physicians and patients display classic Stockholm Syndrome. We have been in captivity so long that anything we get from our captors makes us more beholden to them.
I worry that physicians have become so entwined with Medicare monopoly (monopsony) we can’t imagine anything different. Our greatest wish is ‘to get back to the negotiating table’ and hopefully the pendulum of fiscal prosperity will eventually swing our way again.
Considering that we have not seen the end of cuts, I don’t see any way we will recover until well after 2030. The % increases required to recover to 2012 fees by 2030 would make all other public employees green with envy. And it would bankrupt the system.
Winkler said we’re on a collision course. I wish we’d all admit it and stop trying to defend our dreams or legacy or whatever other motivation keeps us from facing the facts.
Thanks again for your very stimulating comments!
Best
Shawn
“What will it take to awaken the bear; when will doctors fight back?”
The fighting back has already begun in the underground…in our individual clinics and practices. In what the graduating residents are deciding to do with their careers. In what the medical students will be ranking family medicine in their list of residency choices.
It will accelerate with the MOH deadline to accept the changes in the rostered models and, hopefully, the profession will become mobilized when the clawbacks begin.
It does not have to be this way. The OMA could lead the charge and stop navel gazing about the ‘court of public opinion’. Every time I hear that ‘doctors will do everything they can to minimize how patients are affected by the cuts’, I want to throw up. That, to me, is disingenuous and not reflecting what is going to happen on the ground. The OMA, professing this, is leading from behind.
It is time for some hard and difficult language from Central.
Well said, Paul!
Letters to OMA central make a huge difference. As you might know, I sit on the board as a district director. When I get a few emails, I can speak with passion about how physicians are concerned in my area. Of course, I am NOT the spokesperson of the OMA; I do NOT SPEAK for any organization I work with now or in the past.
I feel terribly powerless. I agree that letters to the editor, social media and meetings with MPPs help. But I can’t help wondering whether it’s getting old. We’ve been in negotiations for almost 3 years straight.
I hope your comments about fighting back bear fruit. I’ve seen some amazing grassroots work. We need more of it.
Family practice fees will not recover before 2030 and possibly much longer. I’m waiting for someone to show me how this statement is wrong.
Thanks again for taking time to read and comment!
Best
Shawn