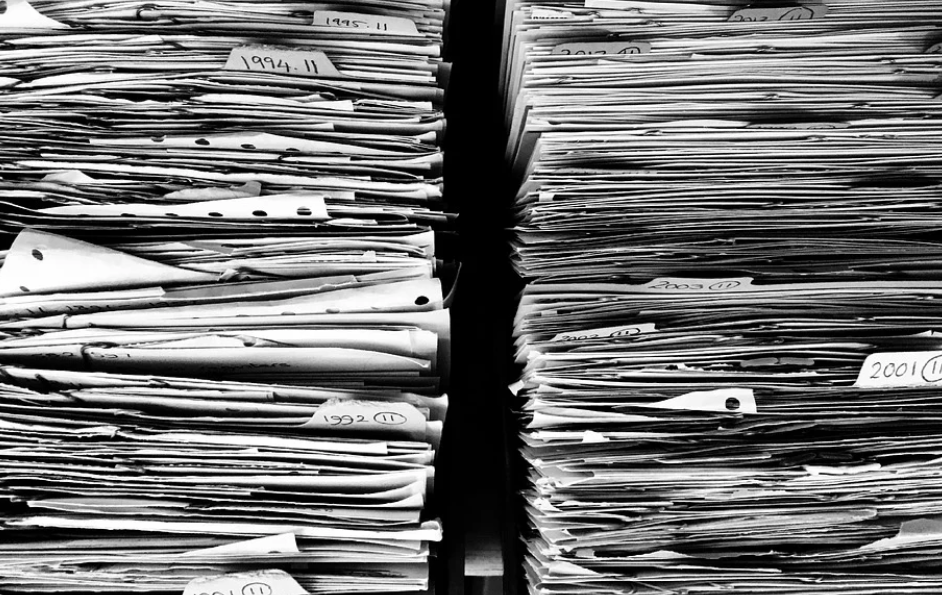
Clinic walls used to sag with special shelves and trays full of forms. Cupboard doors refused to close as forms refused to stay inside. Extra forms always slipped out onto counters and floors, when you tried to yank one out from the bottom of a pile.
A secretary’s job description included being able to answer: “Where’s the form for the new clinic?”
Last time we looked at forms, I aimed at bureaucrats and the heavy loads they tied on doctors’ backs. It was accurate but not entirely fair. Many physicians (most?) love forms and hide an insufferable desire to bureaucratize.
Thousands of Forms
Computers now store all our old paper forms, plus hundreds and hundreds of new ones—over 1,100 in some cases.
One form is for ordering a CT scan at Southlake Hospital. Another for CTs at Markham.
Anything required outside the clinic needs its own form. Hand-written notes will not do.
Inside hospitals, Pre-Printed Orders multiply forms near infinity.
Forms set the standard of practice for all tests, most treatment protocols, and many referrals.
Doctors started designing their own clinical forms for personal use years ago. It started with simple stamps and templates designed to speed the chore of charting negatives—just paste the same idealized note over and over, while adding positives if necessary.
Today, chart-taking excellence means inserting a scoring tool for every clinical question for which a scoring tool exists. The only thing worse than not using a clinical form is not knowing one exists for the clinical problem at hand.
Does your patient feel depressed? There’s a scoring tool for that.
Anxious? One for that too.
Confused? Forgetful? Out of shape? Look in the forms’ list.
Even if you cannot find a form to fit perfectly, you can tweak the patient history a bit. Everyone will think you much smarter for having used a form.
Redundant Forms?
A dozen different versions of a similar form begs for streamlining.
Pray no one takes notice. An enthusiastic manager might convene a committee to help simplify your forms and propel him up the civil service at the same time. Continue reading “Faith in Forms Changes Medicine”