
Women earn less than men.
The latest OMA study adds to studies that suggest the same thing. But the OMA data might also offer clues for how to fix the gender pay gap.
Can we find a solution before it festers and consumes the profession?
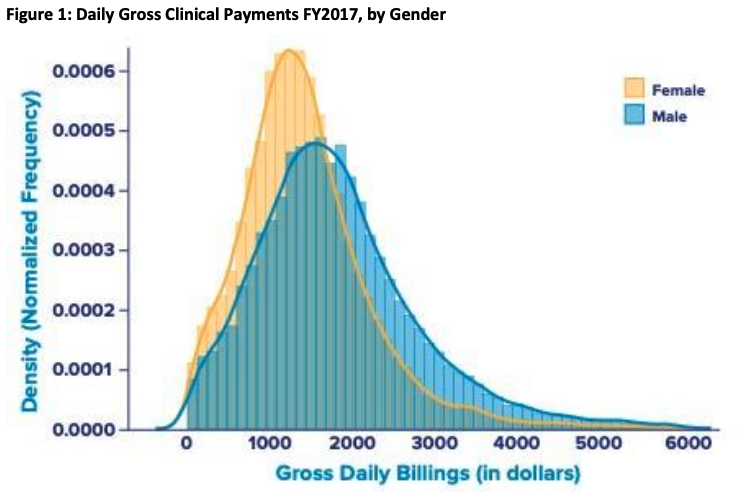
Gender Pay Gap
Some use this graph as forensic accounting. This mindset focusses on ways to assign blame and mete out punishment. It adds another gloomy finding to fuel burnout and depression.
Ample scope exists for debate about causes. This post is not about that. Instead, is there a way to focus on solutions that unify the profession? Does the data suggest a way to improve the gender pay gap?
Successful Women
If we look at the tails of the curves, it looks like both women and men make it to the top, or very close to it.
 This points to two lines of investigation.
This points to two lines of investigation.
First, the graph suggests the absence of a structural barrier. The tails do not seem to end 16% apart.
Of course, maybe those women who land on the tail of the curve have to work 16% harder to get there. Maybe they have found a way to work 16% more hours to earn the same as men who work less? This should not be too hard to find out.
But more important, this tail points to a fascinating area of study.
Some women generate enormous income, over three times higher than average for all doctors.
What makes these uber-successful women so productive? Could these high-earning women teach the rest of us?
What to Avoid
There are a few ways to make closing the gender pay gap harder than necessary.
A. Confuse the gap with relativity.
While we should fix relativity, we cannot turn relativity into a gender debate. It will harm both objectives.
B. Create class war.
Some political visions survive on identifying and fomenting class conflict. Their goal is revolution. It will guarantee docs remain divided (and weak).
C. Fixate on forensics.
Solutions to human problems that demand cosmic justice never deliver happiness and prosperity. Instead of fixing problems, they sour in envy and spite.
We could also debate types of remuneration. But every form has problems: fee for service rewards factory medicine; capitation rewards shirking responsibility; salary rewards on-the-job vacation. And of course, each form can also support outstanding care.
More than Money
Some people use money as a marker. Earning more means they are better people: smarter, stronger, faster, and so on.
Others see money as an emollient for giving up more of their lives (and their family’s lives) than they would have, if they could choose to work less.
But many see money as a fool’s game, a trick designed to make you slave to paying for stuff.
If able, they choose to work less and enjoy things money cannot buy. They spend less and avoid all potential invitations to incite envy. It seems a wise way to stay safe in a socialized, fixed-pie system.
Regardless of what solutions the OMA tries, it seems reasonable to start by listening to the women who seem to have already closed the gender pay gap.
Let’s hope the OMA offers positive, unifying solutions soon.
In a “fixed pie” system aka same amount of dog food no matter how many dogs, it seems like a theoretical exercise to teach more doctors how to bill 500k+ per year!
Good point! So what’s the solution?
(Full disclosure, I’m in the bottom 25th percentile here…)
The fee schedule remains the same within each speciality or field, no matter the gender….this was known when we all chose our paths.
If there is one fee schedule for one gender and another Fee schedule for the other (or the 100+ genders that we are told to exist) then that would be unjust and should be condemned and corrected.
Different choices are definitely a factor.
Some , of all genders, choose to work in the government approved and subsidized system….their incomes remain untouched….some work in government systems , incomes sure with benefits and pensions COVID or no COVID ( work being the pension plan of the pensionless) …some choose in the FFService system…those who chose FFS independence ( of either gender) are noting a massive drop in office visits , hence in their income, even as their overheads rise.
There are older doctors , of both genders, who do not possess the skills to practice virtual visits or comfortable in doing so….their incomes have dropped drastically.
There are doctors of both genders who have health problems that result in decreased incomes.
We see the gender graph….where is the age graph…the years of practice graph…the health/ disability graph?
There are pay gaps wherever we look…if it is decided to close one gap…then surely we should close all the other gaps as well.
Good point about all the other pay gaps, Andris. Very thorny issue to sort out!
I completely agree. Many of the women who complain about the “gender pay gap” admit that they take longer with each patient and also work fewer hours. So why should we penalize those who are faster and work more? Personally, I think that this is a ridiculous exercise: nothing can be more inherently fair that a fixed wage for a fixed service.
Eell said Andrus!
Don Prior
“Gender Pay Gap: A Way to Fix It?”
Why?
Unless you can show that the gender gap is LITERALLY due to discrimination based on gender then looking for a solution is a waste of time and money for the OMA. In fact, it is worse than a waste: it is counterproductive to the interests of most OMA members. Like the pursuit of Relativity (of which gender is just a subset)it will keep the incomes of ALL physicians down.
I would suggest that to be fairest to the consumer, we should let the consumer decide which physician he or she pays. Then those who spend more quality time with patients (in the patient’s opinion) can be paid appropriately.
I am not suggesting an end to our Government Health Care Safety Net. I would suggest that a minimum annual income or something similar would give patients the freedom to spend their health care dollars as they wish. On top of this there has to be a limit to how much an individual spends of their total income on their health care so that no one goes broke because of poor health. Didn’t someone in Canada say something like that a long time ago? Tommy Douglas was it?
Good point about OMA resources, Gerry.
And smart to give the decision making back to patients. We should all benefit or suffer depending on what patients want.
It is a postmodernist fixation to have equality of outcome.
Equality of opportunity is one thing ( hard to achieve but a worthy goal)…equality of outcome is another…individuals are different in themselves and have different goals…some might , for example , want to start a family as soon as possible …others might want to delay having a family…others may not want to have a family at all….once qualified individuals make a myriad of decisions which result in different outcomes, financial and otherwise.
Attempting to equalize outcome, to create so-called “ fairness” is absurd and could lead to tyranny.
“The worst form of inequality is to try to make unequal things equal” ( Aristotle)
All the problems in health care and this fictional ‘gender pay gap’ is being brought up? I had higher hopes for this forum.
Thanks Don.
Good point about diverting energy from all the issues that we need to address. However, I do not think that we can choose to ignore this one given all the energy poured into it. I worry about the impact of the tone with which this issue is being addressed.
Regardless, sorry to disappoint you. It burns bright for many over the last few months.
Best
I agree with your sentiments about the issue. But Don’t shoot the messenger, Don.
One senses that the OMA’s hierarchy is creating or magnifying a problem , empowering the organization to “ solve” them as a way of evading facing far greater problems afflicting the profession.
It is noted that this thread is now in Medical Post, since I’ve been banned from MP for several years, because , I’m told by the editor, I’m “upsetting younger doctors” …I ‘ll continue here, a non woke site.
Choices.
A)
I recall , in the early 70’s, the senior partner at the clinic ( and his wife) owned a high end ski club, he would worry if his billings went up and took an aeroplane full of club members to ski in Switzerland and else where( free of course for he and his wife and family members).His billings were low.
B) A colleague of mine entered medicine to please his parents, in reality he wanted to be a painter.When they died , having a country home in Ontario and another in Cornwall UK, he works in locums on both sides of the pond, essentially to cover the cost of canvas and paint.His Billings are very low.
C)
Another acquaintance of mine, very skilled in medicine, has a love / business of breeding large tropical birds…he left Ontario because hydro costs were too high…he is now practicing out West with a large structure for breeding…his billings reflecting his passion.
D)
I note colleagues of both genders, getting involved in the cosmetic business, working minimally in clinical practice, raking in cash in their cosmetic facility. Their OHIP billings not reflecting their true billings.
E)
I note the movement out of clinical practice of those going into the very lucrative virtual no touch medicine, they are not coming back…their billings are soaring with overheads falling…whilst the incomes of those who remain in office clinical practice are falling and overheads rising.
Distortions due to choices all over the place…the graphs trotted out by the woke gender pay gap advocates not reflecting the choices made by individuals of all genders.
Brilliant summary of present circumstances.
Real problems outdistance woke culture highlighted ones.
Great list, Andris. Excellent point