
 People ask, “What does my Family Doc bill when I go to see her?” This post tackles the most common fee code that family doctors use and how cuts relate to patient experience.
People ask, “What does my Family Doc bill when I go to see her?” This post tackles the most common fee code that family doctors use and how cuts relate to patient experience.
“Do I have pneumonia?”
Imagine you visit your doctor for a bad chest infection. She listens, asks about specific symptoms, rules out other problems with more questions, reviews your family history and performs a physical exam. She orders a CXR and blood work, reviews your allergies and medications, and writes a couple prescriptions. A few days later, she reviews your blood work and x-rays then has her staff call you with the results.
Your visit, tests and follow-up cost $33.70. The fee code is called an Intermediate Assessment, A007, a cornerstone of family practice. Of course, there are higher fee codes (e.g. Annual Physical). They’re billed far less often and require more office time. A007 acts as a benchmark for work in family practice. The OHIP definition reads:
“An intermediate assessment (A007) is a primary care service that requires a more extensive examination than a minor assessment. It also requires a history of the presenting complaint(s), inquiry concerning and examination of the affected part(s), region(s), system(s) or mental and emotional disorder as needed to make a diagnosis, exclude a disease and or assess function. This is a family practice code but should also be billed by specialists practicing outside of their specialty and/or in a primary care practice setting.”
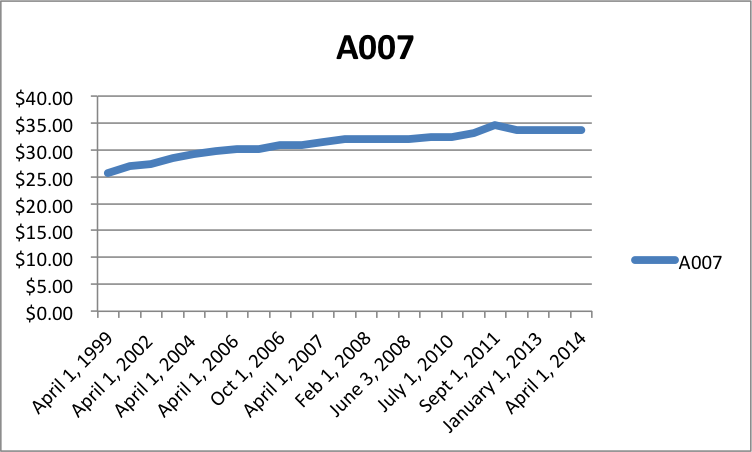
In 1999, A007 paid $25.65. Fifteen years later, it pays $33.70. It increased 1.84% per year – less than inflation for the same time period (1.97%).
Overhead, Hours, Billings
A doctor’s office costs approximately $120-$140,000 per year in Southern Ontario. Most doctors take at least 4 weeks holidays. Therefore, overhead costs $2500 – $2900 per week worked.
A physician must spend 20-30% of her time with office work, not seeing patients. That means 1 day of reviewing labs, charts, and X-rays for every 4 days of time with patients.
Seeing patients generates fees. Reviewing labs and X-Rays does not.
A full time family doctor has 30 hours/week to see patients (7.5 hr x 4 days). Doctors must see 2.5 – 2.9 patients every hour, at $33.70 per patient, to cover overhead.
Most doctors can see 4-5 patients per hour if patients have one, straightforward complaint. With high overhead and 4 patients per hour, doctors earn $37.07/hr. At the other extreme, with low overhead and 5 patients per hour, doctors earn $84.25/hr.
How to increase billings and decrease expenses
Doctors increase efficiency in 4 ways.
- They work longer hours after their office is closed and staff have gone home.
- They take fewer holidays when the office is open. That is, they avoid paying for an office unless patients are in it.
- They decrease overhead expenses.
- They see patients faster.
The first two cause physician burn-out, the third causes staff burn-out and the last cuts time with patients.
Treadmill
Patients feel the biggest impact of fee cuts in less time available with their physicians. Doctors end up trying to shorten visits and book unique appointments for separate concerns.
Primary care reform changed the fee-for-service-treadmill with capitation – paying doctors one fee (e.g., $135) – to provide all care for 1 year no matter how many visits are required. Older patients carry a slightly higher fee and the young a much lower one. But now, some patients struggle to get in to see their doctors; especially if they require multiple visits.
Patient Impact of Fee Cuts
Fee cuts:
- Make the treadmill faster – less time with patients
- Increase patient visits – docs insist on 1 complaint per visit in fee for service
- Make it harder for patients to get an appointment in capitated models
- Encourage physicians to work longer and harder for the same earnings (more burn-out)
After overhead, many family doctors make just over $100,000 per year (every average requires some to fall below the mean). Patients feel legislated fee cuts when they access care. Regardless of how you define what qualifies as a high income, most professionals will try to maintain earnings by working more, running faster, or decreasing overhead (e.g., reduce unpaid services). Patients feel this. That’s more than enough reason to stop cuts.
photo credit: smartchinasourcing.com
I received a link to this analysis from my daughter, who has a family practice in North Western Ontario.
It is clear that the medical community needs a better advocate. The automotive dealership where I work charges shop time at $115.00 per hour.
I recently visited my dentist’s office for a cleaning and a check-up. I was seen for no more than 30 minutes and I received a bill for $247.00.
Your letter explaining the OHIP payment scheme must be better communicated to the general public. If that were so, I am confident that they would be just as outraged as I am. Tax payers pay our politicians 6 figures, they have in many circumstances little or no educational background, this payment does not include staffing costs for constituent offices and assistants while in Toronto where they are supose to be working. I give you an example; our member of Provincial parliment is Sarah Campbell, she was Howard Hampton’s secretary until he retired. A secretary with no formal professional education, and she makes 6 figures, more than a family doctor with a minimum of 8 years education to become qualified. I ask this question with tongue in cheek, WHAT IS WRONG WITH PICTURE?
Thank you, Mr. Habermehl, for reading and sharing a very thoughtful comment!
Doctors almost never need to discuss bills or money during their regular work. Money makes them squirm. Doctors generally feel they have great jobs and hold a privileged spot in patients’ lives. If anything, doctors often feel guilty that they earn a better than average income by working hard.
So with reluctance, I am starting to agree. We need to compare garage shop time ($115/hr) or dental fees ($247 / 30 minutes). I hope to take a stab at it in the next post along with the myth “Docs get a 61% raise”. Tabloid-ish claims made by media and politicians hurt the most.
Thanks again for taking an interest! I hope you can spread the word. Maybe you’d even feel comfortable sending a short email to your MPP if you have a spare minute.
Kind regards,
Shawn
Your comparison is laughable at best. When was the last time you saw a lineup in the waiting room to see a dentist or a mechanic? If your mechanic took 1 hr after appointment time to see your car, you would go to a different mechanic.
You make an excellent point, rx81!
Patients have no control in our current system. They cannot go anywhere else to access care. They can’t vote with their feet like they would from a Dentist or mechanic. Your comment points directly at how the system is designed. As the system runs out of money, it rations care. Wait lists grow. Waiting rooms get more packed. That’s another result of cuts.
If we had slightly more access available than a community needs, then you would find physicians competing for the opportunity to provide care to you. This was once the case 30 years ago. New doctors would buy practices from retiring docs because new doctors knew that they wouldn’t have any patients to see for years if they didn’t buy a practice. No patients = no income. But those golden years of medicare have long passed. Now, patients wait in lines and providers, clinics and hospitals do not have to worry about patient service. There’s always more patient demand than the system can deliver.
So thanks so much for making your comment! While I suspect you were criticizing, it actually aligns exactly with what I’m trying to say. Cuts decrease patient service.
Best,
Shawn
As a fellow constituent and longtime friend of Sarah Campbell, I can assure you that she is much more than just “a secretary with no professional education.” In fact, Sarah holds degrees from Lakehead University in Political Science and Women’s Studies. She has also held many positions over the years on boards and municipal bodies in the Kenora/Dryden area. She has been an active member of the NDP for as long as I can remember, and in my opinion Is extremely qualified for the job she now holds. Peace.
Fantastic comment, Sheena! Thanks so much for disagreeing so politely, offering facts and presenting your perspective!
Be well,
Shawn
Locked up in this comment is for me the reason why this current media debate is missing the point. My average work week is 85 hours. I am lucky to get two full weeks off a year.
So Say I earned $100 an hour for 48 weeks a year (assuming I actually had four weeks off!) then that would amount to roughly $410000 / year!
That would of course include my overhead.
Am I then really such a bad deal? Likely cheaper than any trade the Government use? What do they pay hospital contract plumbers? Would love to know
Exactly! I actually started a post to compare: minimum wage, hourly wages of office staff, allied health, mechanics and accountants. If you use 40, 60, and 100 hour work weeks, the annual incomes get enormous, even without overtime, etc. I feared that, again, people would fixate on annual incomes while at the same time scoff at the 100 hours per week. Most people cannot get their heads around such a number.
Thanks again for sharing your experience!
Shawn
Excellent viewpoint!
I still like my husband’s comparison with politicians….whole seasons of paid vacation, full benefits, and THEY get to waste as much of the taxpayers money as they want! WE, as devoted, good family doctors, will be penalized in years 2 and 3 for the overspending of our colleagues. Hmmmm….I think all politicians should get the same treatment of their salaries when their colleagues overspend their budgets!
I’m sorry to disappoint all those who say this is all about health care quality and not about our personal income, but after 25 years of debt just to run a good and caring family practice, for me, it is now all about the money…..because I’ve never NOT provided good health care!
It’s another of a series of insults and slaps-in-the-face by the Ontario government.
Trying to stave off depression,
Donna
Great idea! Everyone cries for accountability, but no one wants it for themselves. Time for a referendum? 😉
Don’t get too down over this, Donna. You do great work for patients every day. In the end, they will vouch for you. The ‘end’ may take some time to come about, but they will demand proper access to your care.
Shawn
Hello;
I am a health care professional, although I am not nearly in the same category as a Medical Doctor or a family physician.
I understand the mandatory overhead costs, as I imagine that they are more expensive versions of my own (liability insurance, general insurance, membership in professional associations and colleges, annual continuing education and professional development etc.) however I still can’t even begin to reach what you’ve got listed as weekly overhead!
Most family doctors are in essence small business owners, or in partnerships with other doctors to create a bigger small business. Perhaps these overhead costs could be reduced through treating the practice like a business, so that it is not the time with patients that suffers. Seeing 4 patients per hour doesn’t sound like an adequate amount of time to treat patients, however if this is what is required to break even, then the overhead has to change!
This isn’t to say that the funding shouldn’t be cut, but having a yearly raise in fees of %.1 percent below the inflation rate doesn’t seem drastic enough to cause such a discrepancy between income and overhead.
One last comment; In this economy, regardless of the argument that doctors have SO many years of education to pay for, a yearly take home of 100k doesn’t sound that terrible.
Thanks Alana!
Great comments. You are correct – overhead must come down. Family doctors usually need 2 full-time staff to help, or a minimum of 1.5 staff per physician in a group practice. Office staff earn $20-$25 per hour (less if benefits included). That’s $37,500-$46,875 per staff for 37.5 hour work week, but many doctors staff their offices for 50-60 hours per week. A conservative estimate of staff costs for a solo physician is $75,000-$93,750. In a group practice where doctors use only 1.5 staff, it would cost between $56,250-$70,312.50. That’s just for staff. Lease, equipment, heat, hydro, cleaning, supplies, phone/fax, internet, computers, office insurance, etc, etc, etc add many more thousands per month.
Again, the best way to decrease the % that overhead eats out of total earnings is to work more, much more. Trying to save a few $$/hr on staff ends up costing more later.
You mention inflation. Overhead costs have outpaced inflation with the cost of new technology. Paper, fax and phone-lines didn’t cost as much as all the gear and support required in a modern office.
Finally, you mention that $100,000 doesn’t sound too bad. I agree! Heartily! But with TTC drivers toping out around $80k and higher, with full pension and benefits, and early retirement, I wonder how we can justify such a low value placed on medical care? Dentists bill $247 for 30 minutes according to the last comment.
My main concern is for people to know that 1) most doctors are not ‘loaded’ like politicians want you to believe, and 2) fee cuts impact patients. As a patient, you will feel the difference. And that’s not going to benefit you.
Thanks again for diving in! I appreciate your suggestions and willingness to push back a bit!
Best regards,
Shawn
Dear Shawn and Alana,
Shawn, you neglected to report that without a pension plan, UI for illness, vacation pay, not being paid while you’re taking vacation if you’re in a FHG eats into that $100,000…..by the way, 60% of that will go to taxes…..
So after we pay for disability insurance (which will only kick in if we’re off work for 30days, as the premium for anything else is punishing), liability insurance, office insurance, pension plans and investments, and TAXES….there is NOTHING LEFT!
Cheers,
Donna
Well said indeed. You might also consider that you have to make all your earnings in fewer years compared to someone with less training. The higher-income-in-fewer-years approach attracts far higher tax rates compared with earning a lower income for a longer career. That’s why my Dad could retire as a teacher at 52 on a full pension with benefits and have no debt. He was frugal but also benefitted from starting work younger.
Oh well. We never went into this for the income. But we didn’t go into this to get slandered by politicians either.
From start to finish, we need to keep this about patients: how do cuts impact access, time with physicians, attitude of physicians towards practice in Ontario, etc. All these things, and more, will change the way patients experience their care.
Thanks again! I’d better get working on another post about our “61% raise”. 😉
Best,
Shawn
Oh, Shawn, I look forward to that one!!
Thanks!
Time to work on charts,
Donna
Don’t hold your breath…but I think it will be fun!
Don’t work too hard.
Shawn
Wow! When I subscribed to read all further comments on this thread, I didn’t expect to see so much!
As a non-physician allied health care provider, I agree with many of the things being said here but some of the opinions and comments frustrate me as as both a health care practitioner and as a consumer.
I do not believe that the high cost of obtaining education and becoming a doctor is an argument for a higher take home after opening practice. Many professions have this struggle, mine included, however I think the struggle should be with lowering cost of education, not increasing cost of product/service. Debt is undertaken knowing that income is not guaranteed.
Also, the idea that doctors don’t have a high income because they need to pay their own pension, benefits etc… Well welcome to the club! We are living in an era of self employment, where these things are expected. Perhaps the idea of employee based family practice is something that should be explored if this is such a problem. Remember that self employment also comes with many benefits as well as drawbacks.
Isn’t it also great that a doctor need not spend time or money (for the most part) on marketting to achieve a full day of work, and that qualification is never questioned even when it should be!
This entire thread of comments went very far from patient care, and unfortunately went the way of so many arguments in my (young) generation: employment and wage entitlement.
Thanks again for sharing your thoughts, Alana.
I always value strong opinions shared with conviction, so I appreciate yours posted here. Sometimes, however, our audience teeters on the edge of personal crisis.
Having dug out from under a mountain of school debt myself, I know a little bit about what some of the students and residents are sharing. But they have it much worse. Students and residents shoulder $200-300,000 of loans and can just barely see the end of 10-12 years of university around the corner. Without warning, the government kicks the chair out from under them. They get a 30% pay cut (yes, 30% for new grads), get denied access to the care models they trained in, cannot get a job in their specialty (especially for surgeons), and face looking for jobs in another province away from their family.
While the patient impact will be significant, the impact on these students is truly tragic. Canadians built Medicare to prevent patients going bankrupt from medical expenses. But we seem much less compassionate for students who’ve given up their young lives training to provide care for us.
So, I would tread extremely carefully in using ‘entitlement’ around medical trainees right now. They are under attack at perhaps the most vulnerable time in their lives, when it’s darkest under their mountains of debt. Tread carefully indeed.
Shawn
Hear, hear!
As a primary care physician in Ontario, I couldn’t agree with you more Dr. Shawn. Tread carefully indeed. The future looks so bleak for Ontario physicians and patients.
Thank you, Yasmin. Premier Wynne will have dismantled Medicare in Ontario. I do not know that we will recover without building up a substantially different approach.
Thanks for taking time to comment! Readers love reading your comments!
Cheers
Shawn
Dear Alana,
Sorry to disappoint, Alana, but this whole issue is about money. We are talking about the horrible deal the government just laid upon us for the next 3 years. I don’t know what you do. We are saying, as family docs, we don’t work from 9 to 5. Every hour I’m awake I am thinking of patients, AND I AM RESPONSIBLE FOR THEIR HEALTH. With EMR, I am connected all hours. I work on charts from 8AM to 9AM, see patients until 6 on most days, go home to eat, work again from 8 to 11……so if we’re talking hourly rate, I am in the negative. But it’s not even about the time spent data-entering, its the responsibility we take on. Compare to a politician…..making maybe the same salary as we do. They get to take most of their money home….little overhead. And they get plenty of paid time off. They waste tax-payers’ money (just like us?) and they aren’t going to have their money withheld in years 2 and 3 if they overspend their budget. How would you like that, Alana?
Alana, it’s about the unfairness of this whole contract, and the devaluation by the government, the slap-in-th-face for young graduates and new docs who hoped to set up good old-fashioned family practices in their home province of Ontario. They just won’t be able to do that.
As I said, I love my job, I wouldn’t change my job for the world, but it is definitely undervalued. Sorry if that offends you, but we cannot help but feel this way.
Donna
Well said, Donna. Well said, indeed.
Thanks so much. I can add nothing to such a thoughtful, passionate, articulate note. I hope many others read it!
Shawn
Tuition is 25000 a year for four years.
Alana-
You mentioned that seeing 4 patients per hour seemed like a lot, but we should continue doing so if that’s what we need to do to cover expenses. What is not mentioned here is that there are enough patients waiting to be seen for us to see 10 per hour and not get through them. You’re right that the time is not adequate but billing is only a small part of why I rush through patient encounters- if I didn’t, the majority of my patients would suffer from lack of care. When I work at walk ins, I take no breaks in an 8 hour shift and rush from patient to patient, still only seeing 45 in a day. Many of those patients wait 2+ hours just to see me for 10 minutes. Our patients need better care but with more cuts the care is sure to get worse. I, for one, will start taking lunch breaks!
Great addition to the thread! Thanks so much for taking time to share it. People love to blame doctors’ greed for working quickly when most of us would love to slow down. Patient need and long waiting drives most physicians to work faster, not greed.
Thanks again!
Shawn
Dr Whatley,
Eureka, and BRAVO!!! This is going up in both my exam rooms and at the front desk! This is awesome! I am sending your link along with my letter to the OMA.
If only every intermediate assessment was as easy as the one you described!
Many thanks,
Dr. Donna G. Mahoney, MD, MSc, CCFP
Woodbridge
Thank you, Dr. Mahoney, for your encouraging comments!
I feel relieved to hear that other physicians support this description of family practice. From comments here like yours, and many others on Twitter, it seems like most physicians find the post to ring true. Phew!
But more than that, I am thrilled to hear you are passionate about sharing your thoughts with anyone who will listen. As physicians, we find it more natural to reach out and help versus stand and fight.
Most of us have spent the last few decades apologizing for wait times and poor access. We apologize that patients need to rebook, or that we have to rush along to the see the next patient. We need to help patients understand that this has been designed by a central authority. They makes sweeping changes that we spend our lives apologizing for. Patients deserve better.
Thanks again for reading and commenting!
Highest regards,
Shawn
Dear Shawn,
Silly that we are always apologizing. Maybe it’s just our Canadian ways. I’ve decided I’m going to put more value on myself and my work and be more aggressive with billing patients for renewals and phone calls and letters. I’m often “too nice” and slough it off, but why? A lawyer would never do that!!
I’m clearly not in it for the money, but I do have to balance my books, and I have to stop feeling guilty for billing for the paperwork and my time.
I really thank you for this letter, Shawn. I think the OMA, in an aggressive campaign, should publicize the costs of every test, so that patients understand why they shouldn’t be requesting them so readily. It’s not enough to tell them to go to a website which teaches about evidence-based medicine. They’re not going to do it. It needs to be IN THEIR FACE, and instead of that silly campaign about how much we care for them (my patients already know that) they should be telling them in real numbers what their health care costs.
Thanks again,
Donna
Another excellent comment, Donna!
I totally support you putting more value on you and your work. Patients benefit from that attitude. There’s no way you can provide outstanding care and service if you are feeling beaten up, undervalued and ignored by the system. Patients benefit from happy, fulfilled doctors. Disgruntled physicians do not give great care.
I struggle with billings, codes, money and numbers. I don’t know if patients want to hear about it, either. I feel forced into talking about it by media and politicians who make us cower with slander and hyperbole. Having said that, it seems there are more patients wanting to hear about the numbers than I ever realized. Maybe times have changed? Maybe we need to post every little last detail in our offices like you say?
As for billing for things not covered by OHIP, people value your service by the amount it costs. While people thank you for not charging for notes, etc., your services get taken for granted. While I grumble at having to pay my lawyer for notarizing ($20 for a 1 second stamp), I know it cost the lawyer hundreds of thousands to get to the point where he could press a stamp and charge $20.
Again, great comments all! I’m humbled by the wisdom out there. When the experts on the front lines speak up, the truth will come out. Keep speaking up!!
Best regards,
Shawn
Very well written Dr. Whatley and I will be sharing this article with my classmates. After reading your article, I am even more saddened by the fact that primary care and family physicians are being hit the hardest with these cuts.
Thanks so much, Mathew. I really appreciate you taking time to read, comment and share this. I hope it rings true.
Please feel free to post negative comments, too! 😉 If you ever feel the message comes over too shrill, off base or factually wrong, please let me know. I care most about people thinking differently. If the medium distracts from having readers engage with a concept, I want to adjust it.
Again, thanks for commenting!
Warm regards,
Shawn
I’m a soon to be family medicine grad and I’m just so upset with the changes our government is proposing. New grads doing family medicine who hoped for income stabilization during their first year will likely lose anywhere from 30-60% of what they would have earned. Like most people I have a new mortgage and bills. Unlike most people I have $200,000 of debt and have made numerous financial sacrifices to get to where I am with no pension, vacation pay, benefits or paid vacation in my future. My income needs to account for these.
Unfortunately, this policy has has consequence that will fall on patients. I won’t be able to go out and start a family health team and roster patients. This won’t allow me to balance my books – there’s no incentive now to be a good family doctor. Instead I’ll have to do rushed fee for service walkin and ask patients to only bring up one concern lee visit. This is not what I got into medicine for.
Additionally, our most vulnerable patients who are so complex are having their attached health care dollars taken away. I worry that they will have a harder time getting care. Taking away any incentives to do after hours and weekends is going to push everyone into the emergency rooms where it costs 10-20x as much to treat them there. These policies are short sighted.
If the government wants patients to get care and save money then they will have to pass the buck to taxpayers eventually. Or out of necessity expect private practices guaranteeing access to pop up, there will be a demand for it.
It’s a bad time for new family med grads and I hope our future is brighter and family doctors, and physicians in general, can really be part of the solution for optimizing care and reducing money in the system without impacting patient care.
Mike
Wow, Mike. If only everyone would read what you just said…better yet, if they could sit and visit with you!
You nailed it with your comments about how this will impact patients. You, our new generation of physicians, will be forced to work faster, longer and harder just to get out of debt let alone start thinking about saving for retirement. You will be in survival mode for at least 10-15 years. Times were much better when I started in 2000, but it still took me 10 years to dig out of debt. Of necessity, you will not be able to afford to accept tonnes of older, sicker, more complex patients.
You’ve probably already thought about this: Where else could you find a job? Where else could you practice medicine in a way that supports putting patients first?
Other provinces don’t treat doctors so poorly. You’ve got your whole career ahead of you. If you stay and sell your soul by practicing a style of factory-medicine you don’t believe in, you will die inside, and patients will not get as good care as you might have given otherwise. Even if your income somehow goes up in Ontario, our government has taken more and more centralized control of medicine over the last few decades. Other provinces do not tell you how to practice medicine as much.
I know how you feel. I started a tiny rural family practice last fall. My numbers are growing slowly, but I refuse to jump on the factory medical train. I want to spend time and dig into all the issues patients have at each visit. I hope you refuse to compromise what you believe to be good patient service, too.
Keep spreading the word! Our only hope is to have voters speak up.
Highest regards,
Shawn
Dear Mike,
PLEASE don’t despair. Please remember that family medicine is still a great and noble profession. Despite our complaints, the job is still very fulfilling. Make it fun, enjoy your patients, and they will respond back. If you are nice to your patients and treat them with respect, it will be a satisfying job.
Hopefully you’re not really in it for the money, because unless you’re into volume, it isn’t lucrative here in Ontario. It never was (25 years of changes has been difficult and frustrating to bank balance) but in the end you want to enjoy your job. You’ll make enough, but in Ontario, in family medicine, you’re not gonna be rich practicing to stay sane and happy.
Love your job and family first.
Donna
Brilliant comment, Donna! You are right. Many of us would do this job for free.
Starting out feels overwhelming enough without all these extra stresses thrown in! It gets better if you live really frugally. My uncle said, “Live like a student for at least your first year of work.” I’d say, “First 4 years of work.” That way, your financial stressors won’t distract you from great patient care.
Thanks again for sharing, Donna!
Best,
Shawn
As a R2 in family medicine I feel exactly the same as Mike. The recent changes that the Ontario government is imposing on physicians demonstrates how little respect they have for our profession. Unfortunately the coverage I have seen has not brought up the changes that are going to affect predominantly new grads.
As far as I understand, the income stabilization program has been removed and new grads are no longer allowed to join FHTs/FHOs and roster patients (other than in remote regions). This forces new grads to work in a fee-for-service model.
Income stabilization is incredibly helpful for a new grad. If a new grad is building a new practice (or joining a practice) and building a patient roster, they will need several patients before they have a positive cash flow. The income stabilization program ensured that physicians could build up a practice and still have enough take home to eat and pay off interest.
Fee-for-service has its benefits and drawbacks, most of which have been mentioned above. Overall complex patients tend to be overlooked in a fee-for-service model and physicians are essentially forced to either push through simple visits (ie. refills each month to have quick and easy appointments to bill) or to find other sources of income (block fees, non-OHIP covered services) if they want to make money and take care of complex patients.
Furthermore, a quick comparison of the OHIP SOMB and other provinces SOMBs (in particular Alberta’s SOMB) will demonstrate that several common billing codes pay significantly less in Ontario. Previously this didn’t matter as much in a patient rostered type model, however, with new grads being forced into fee-for-service models this makes a huge difference in realized income.
I feel very fortunate that I have the opportunity to “vote” on the policy by simply leaving the province. As a new grad I would prefer to serve a province that respects the work and value that I bring to my community. Unfortunately, several of my colleagues are stuck in Ontario due to family and mortgages.
The Ontario government have essentially balanced their healthcare budget by picking on the group of physicians (brand new family medicine grads, usually with > $150k student loans) who can afford it the least. This is akin to the bully in the playground preying on the kid who can’t defend himself.
Matt, thanks so much for your clear, calm, but dire note!
You’ve been honest enough to describe exactly what’s going through a resident’s/new graduate’s mind. Scary. I totally support you finding a province that allows you to practice in a primary care model that allows you to deal with all the problems a patient might have instead of rushing them through. If you have a choice, why wouldn’t you go to a province that values your training? If you set up somewhere else, there’s a good chance you might spend your whole career there. Ontario loses out. You benefit by being respected, working in a way you can support, earning a little more and paying far less taxes. Patients benefit from a doc that doesn’t need to rush everyone through appearing harried and disconnected.
Thanks again. I hope people get to read and seriously consider what you’ve written. Keep telling your story; maybe the government will relent.
Highest regards,
Shawn
Great article. Is the 30 dollar fee the only thing you get or do you have an annual salary plus the fees you charge? Thanks
Great question! For those billing only fee-for-service (FFS), all earnings come from codes like the A007. By the way, A007 is the most billed code in the whole province at over 18,000,000 submissions. The next most frequently billed code is just over 6 million submissions.
Since primary care reform, a number of different payment options exist. Options have more or less blending of an FFS element (at lower fee rates) all the way to a full salary with no FFS portion. Even when the FFS portion is almost entirely removed from a particular funding model, doctors still usually submit a fee code so that services can be tracked. In capitated or patient-enrolment models, doctors get a monthly stipend determined by the number of patients enrolled to them and bill reduced fee codes.
Sorry. That’s probably too many details for your question. Short answer: pure FFS = no salary at all. Blended models = some monthly payment based on # of enrolled patients plus some payment for each service provided.
Either way, the A007 fee code description remains a benchmark that guides people’s thinking about primary care services.
Thanks for asking!
Shawn
I am also a PGY2 in family medicine. Some of my colleagues have already outlined my situation quite accurately above, and I wholeheartedly agree with them. My three points to add to the conversation are:
1)Directly due to the manner in which the cuts will affect new graduates in family medicine many are in the process of cancelling their plans to start a family practice in Ontario.
The one alternative discussed above is to move to another province, but for many this is not ideal as we have partners/children/family to consider. The second solution that I am seeing is that we are opting to do only non-office based family medicine such ER, hospitalist, palliative care etc. Personally I had planned to start my office based practice July 1st, but this has been put on hold, and I am exploring hospital based work only. Common sense tells me this will not be a savings to OHIP as patients who would have been rostered to a new physician July 1st will now continue to access expensive ER services.
2)Although I understand the sentiment, the expression “Many of us would do this job for free” is very unhelpful and furthers the divide between new graduates and established physicians. I am not ashamed of saying that I will not do this job for free, I will not even do it for the vastly reduced compensation that is now being offered. Quite simply I can’t. I have $260,000 debt from medical school, 0% of my mortgage paid off, 0% of my retirement funded, and all the same household expenses as everyone else. I love the work I do, but I am governed by the same fiscal realities as everyone else.
3)The Ministry should make public what they feel is fair compensation for a family physician. Take into account debt load, overhead costs, a hypothetical 40hr work week and standard billing codes such as A007. Show new physicians and the public how many patients I need to see each week to achieve this “fair compensation”. How many minutes does this leave for each patient? I think the results of this would be very revealing.
Thank you for furthering the discussion,
Kevin
Thanks for sharing your excellent note, Kevin. And for bringing us back to reality.
You make solid points about the financial realities of training and working as a family doc. You should not expect to work for free. Only after you’ve paid off your debts, put your kids through school, and saved for retirement will you have the luxury of ‘working for free’, sometime in your late 60s or 70s.
You add another important point about how this will impact patients. New grads will avoid office practice. You won’t be able to afford it. Patients will feel the decrease in access, especially outside the GTA.
Thanks again for sharing! Your thoughts on ‘fair compensation’ get into a debate on political philosophy; one I love, by the way. I think there’s hope if we can all go against our usual habits and all speak up about this mess, no matter how uncomfortable we feel talking about money.
Brilliant comments!
Best regards,
Shawn
Dear Kevin,
You are absolutely right!! I don’t know where that There is no way that anyone should so this job for free! In practice for 26 years. I love the medicine, HATE the data-entry which takes the majority of my time.
No, no matter how you practice medicine, it is tough, challenging and needs to be compensated well! Not even to make up for the astounding debt but to pay for the valuable expertise you provide. It seems the government forgets about that value, certainly doesn’t appreciate it!
I feel very sorry for you residents! I feel sorry for me as I’m thinking I can never afford to truly retire!
PLEASE send all your constructive thoughts and ideas to the OMA negotiations team ASAP. I know it might be a waste of time but it’s all we have. They certainly haven’t done much other than to waste our money on dumb campaigns telling the public how much we care. And telling US we should be educating our patients about the costs of health care….like we have time. GRRRR!
Sadly,
Donna
Donna,
I completely share your sentiment! In everything you say! OMA is wasting our money on a ? Spread yhe word on doctors, as if we already didn’t know campain, offering no course of action for us! We need to press them to make our voice heard! I was planning to open a private practice. There is no way that is going to happen! I completely hear the newly grads here, I have been practicing for 7 years and since I started, I have had nothing but cuts to the income! My question is: how long will this go? What is the long term plan? There is nothing that protects us as govt employess from unilateral cuts in the future. Nothing that protects us from a govt that may eventually ask us to work for food and water!
I’ll let Donna reply, since you addressed this to her, but I just wanted to thank you for taking time to write! Many share your desire for action. Best, Shawn
This was very well written. You should consider forwarding your comment to the ministry. I think they need to hear more things like this.
Thanks! I appreciate you reading and commenting!!
As a medical student in clerkship, in the process of deciding my career path, I can say that the cuts to family medicine are a significant new deterrent to choosing Family over almost any other specialty. In my experience so far, FFS practice all-to-frequently leads to burned-out, cynical docs who resent their patients for being the tiniest bit complex. The cuts will not change this for the better, and I do not want that future for myself.
I find this all very sad, because I truly believe that family medicine is the most important – and potentially most personally rewarding – kind of medicine. But financial realism creeps in, and now I find myself having to “sell out” and consider which specialties/ practice model will allow me to enjoy a reasonable lifestyle and retire before 70, rather than choosing based on what I WANT to do. As was mentioned earlier by one of the very perceptive residents, this is not what we signed up for when we decided to become doctors. This was supposed to be a vocation, not a job; a life dedicated to patients, not to paying off our bottom line just to keep food on the table.
Shawn, I highly recommend that you forward your analysis to the OMA PR folks. This kind of hard analysis is what the public needs to see, to truly understand the impact of cuts.
Hey Brian. Thanks so much for sharing your perspective from clerkship! I hope you are enjoying it.
All your comments about FFS, burn out, cynical physicians and complexity hit home. Too close to home for many of us I fear. I know you will find a spot in medicine that matches your unique talents with a practice pattern that needs them. In a way, you are much better off learning about this now, while you can still make changes to your career plans!
BTW, the OMA PR folks put this post on their FB page generating several thousand views in 2 days. They are very supportive. Sometimes we can share a very different message from the trenches than OMA central can say as a corporate entity. They need to hear stories like the one you just shared! They need that far more than anything I’ve written. Your voice is powerful!
Thanks again for commenting!
Best regards,
Shawn
A very useful breakdown. Ontario isn’t even the province that’s worst off; in BC the A007 is called a 0100 and is 10% less at $30.15. Family doctors who choose to work in cities like Vancouver also have a higher cost of living. It’s past time doctors across Canada are reimbursed at least the cost of inflation.
Thanks so much for sharing the BC experience, Dr. Moore!
I wonder if we need a discussion that compares fees doctors bill with other bills voters pay?
We train keen, workaholic students, who have a streak of self-masochism, and put them on a treadmill designed to encourage unending patient need. Caring doctors keep running to meet as many needs as possible. Then the peanut gallery slams doctors’ incomes as evidence of greed. In all of this, we try to stay compassionate knowing that the treadmill harms patients even more than doctors.
I fear the trend in Ontario and Quebec will spawn if governments get away with treating physicians with disdain.
Thanks again for sharing your comment!
Shawn
Hello!
I am not a Doctor or nurse, I don’t worry about their pay cheques. I am a mother of 2 boys that have relied totally on the many doctors and nurses, hospitals etc. There is not any part of the health care system that we have not used. In Kenora and Winnipeg! The doctors went above and beyond many many times to keep my children alive! Calls at 10 at night to check on them to meeting me in the middle of the night at the hospital! This is far beyond their pay hours and only because we got quality care did we keep my older boy alive! And when my 15 year old passed away the Doctor on call at emerg called our Doctor at home to come and he came knowing that he would not be paid to sit with us while we took our son off life support and sit with us and grieve and make sure that we were ok as well! The nurses were incredible! Making sure medical things were being done without us feeling like they were getting my son ready to die! I agree with any pay increase to Doctors and nurses (on any wards) getting a pay raise. I would not want to even do their jobs let alone be underpaid for it! I guess you have had to actually need the services before you appreciate what they do for you!
What a powerful story, Theresa!
Thank you SO much for taking time to share it here. In the midst of unspeakable loss, you received compassion from all your care-givers. Your story describes why we went into medicine; to be present and helping when people need it most. I hope your note encourages others as much as it has me!
Gratefully,
Shawn
Dear Theresa,
I can’t begin to thank you for your letter of understanding. Your insight is remarkable, to be able to see the worst part of our jobs from your point of view. And it isn’t that part that I even think about being remunerated for…that truly comes from the bottom of my heart!
I am so sorry for your loss and hope that you and your family are coping as well as can be expected.
With heart-felt respect
Donna
I’m with you until your concluding paragraph.
The average family doctor in Ontario (based on 2010 data, but it can’t have changed that much) makes over $200 000 a year after overhead. Check out this excellent paper:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3517870/
So I am not sure how you arrive at the following: “After overhead, many family doctors make just over $100,000 per year.”
There is a fifth option that you don’t mention, which is that doctors could choose to make less money, without impacting patient care. I agree that most won’t choose to do that, and will instead choose to compromise things in any of the ways you enumerate. But that is a choice, all the same.
That aside, some of the cuts do trouble me, especially the shift away from non-FFS models.
Great comments, Ryan! Thank you for challenging me on that last comment.
I agree, the logic falls apart if we read through in a mathematical approach following the tone of the whole piece. I should have switched gears and put in some linking thoughts. I was attempting to emphasize that within the ambit of family doctors, many earn much less than the average. Furthermore, the calculations are based on only those physicians earning more than $50k per year to eliminate part-time and semi-retired docs. Finally, I was thinking of all the docs on income stabilization who have generous overheads. Most of those MDs work in groups, however, and try to share as much overhead as possible. Income stabilization will disappear with the cuts.
Overall, hard working, full time family docs should be able to earn the averages in the literature, as you correctly point out.
Thanks again! I’m humbled by all the amazing content in the comments. I sure hope folks find time to read down this far! 🙂
Best regards,
Shawn
There is absolutely no way family doctors are only earning in the 100k territory. I know of family doctors who are easily clearing 400k every year.
Skilled physicians are able to see 7-8 patients per hour while maintaining standard of care. They also have strong enough business skills to minimize overhead.
Thanks Michael! You’re right. For every average, there are those above and below the mean. Again, your 400k number is gross billing and 130k overhead comes out of that. “Skilled physicians” can definitely see 7-8 patients per hour if they rush through single issue, simple problems. There’s no way the most skilled doc in the world can get through even 3 elderly patients with dizziness or fatigue in 1 hour.
Again, thanks so much for sharing your perspective. I’m trying to share the perspective of someone on the inside.
Best regards,
Shawn
I will bet those doctors seeing 7 to 8 patients per hour are burnt out, miserable, (skilled? hopefully not missing vital information). That’s not “family practice”….that is walk-in, single issue visits. So if they’re billing A007 intermediates, they are the docs who are draining the system. They should be bililing A001 only.
I’m not saying that kind of doc isn’t needed. That’s not family practice though, dealing with more complex problems. That’s what we’re trained for. If OHIP wants me to stop that kind of care, I will see 7 to 8 patients an hour. So sad!
Donna
Well said! Thanks, Donna.
enjoy your 6 minute visit with your Doctor.
I am sorry but I don’t even understand why people are complaining about the wages of a Doctor! Complaining about wages of such a valuable service when (trust me) at some point in your life you will need these services! You will want them to take the time to explain everything and every option and it will take longer than 5-10 minutes. Let it go. There are far more things to worry about than if your Doctor got a raise! You can only benefit from it with better care. Again you will one day need these services and compassion and care, because death and disease does not care about income!
I only wish everyone had your experience, Theresa! Unfortunately, most voters have never need the care you’ve received, so they don’t value it. Thanks again for taking time to read and comment! Greatly appreciated! Shawn
Hello. Thank you for taking the time to communicate with the general public about physician compensation. As someone with many physician friends and family members I know how uncomfortable physicians are with speaking about this subject. I have two things to add to the discussion. First, please provide all relevant details about physician compensation, especially when you include benefits when you talk about salaried workers. It is valuable to learn about the overhead costs but you also need to be transparent about the impact of being incorporated as over 90 percent of physicians are. According to the MD Management web site there are enormous financial benefits to being incorporated. The corporate tax rate is much lower than the tax rate salaried workers pay and there are many ways to reduce taxable income, such as by paying children or spouses to do work and other special arrangements. The result is that take home pay is much higher per $100k for incorporated physicians than for salaried workers making that same amount and it would be fair to point this out.
This brings me to my second point. I am very concerned that so many of our public services are being eroded. I attribute this partly to the low tax mentality that a variety of parties have been successful in instilling in the public. I invite physicians to band together with other public servants to encourage our governments to stop cutting services and raise taxes – especially corporate taxes, which are currently the lowest amongst the G8 countries – so that we can properly fund the services we, as a society, need.
Thanks for bringing up another common misconception, Tammy.
Incorporation serves as a tax deferral for those doctors able to save after expenses and costs of living. All the other provinces allow MDs to fully incorporate professional practices, as far as I know. Ontario only allows limited incorporation which significantly reduces the corp. benefit. I’m extremely grateful that Ontario finally agreed to give us the benefit that doctors have enjoyed all across Canada for many years. But don’t try to make it sound like it’s a ‘benefit’ like a pension plan, dental or medical benefit.
You ask to raise taxes. I wonder, do you draw an income from the government? In Canada, 1/3 of citizens draw incomes from government or government run industries (e.g., education, healthcare); almost 1/3 receive some sort of benefit from government; 1/3 generate income from something other than government. With so many citizens either paid by taxes or receiving benefits from taxes, I’m not surprised to hear you call for more taxes. Public services decline when countries run out of money. Countries run out of money when income-generators (individuals and businesses) get over-taxed and over-regulated so they can no longer support the gigantic state machine.
Thanks again for sharing your thoughts.
Regards,
Shawn
Hello. Thank you for your reply. I am so impressed that you are taking the time to keep your blog so active and to write so many thoughtful posts.
To your last point, yes I make my living from government coffers just like you do. I feel that we all benefit when our public services are well-funded. Well-paid doctors – and teachers and other public servants – are good for society. But sustaining this pay does require a proper level of taxation.
As for the benefits of incorporation, the MD Management Web Site shows the impact of incorporation. The bottom line is that by splitting income with children and spouses and using other tax planning mechanisms you can pay a lot less tax. Here is one quote from their web site: “So, just to recap, we went from a salaried physician earning $300,000 per year and ending up with $200,000 after tax, to an incorporated physician earning $300,000 per year and ending up with $255,000 in their pocket. That’s more than a 25% increase in take home pay.”
See more here:
https://mdm.ca/wealth-management/investment-management-strategy/investor-education/transcripts/incorporation-transcript.asp
As we read in this previously cited paper
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3517870/
the average after-expense net income of Ontario physicians in 2010 was $240,000 so the math from MD Management could be applied to this lower number, but it still speaks to the benefits of incorporation.
Please don’t take this the wrong way: I feel that doctors need to be well compensated. But I would also like to see an accurate and balanced portrayal of the current situation. And I would really love to see physicians joining others in calling for well-funded public services.
Hello. The $240,000 figure I included above is the estimated mean net income of physicians in Ontario in 2010, not the average. Sorry for that error! I do encourage folks to read the whole article for themselves.
Thanks Tammy,
If incorporation is as good as you say, why have so many physicians not incorporated? Are they just misinformed?
Your bottom line conflates income splitting with incorporation. “The bottom line is that by splitting income with children and spouses and using other tax planning mechanisms you can pay a lot less tax.”
A physician can income split without incorporation, and many have done so for years. As for “tax planning mechanisms”, Ontario specifically limited medical corporations to only the practice of medicine. Other provinces allow medical corps to have non-physician shareholders beyond adult children and to engage in regular business activity like typical, full-blown corporations. This cannot happen with medical corps in Ontario. Doctors can only pay dividends to adult family member shareholders. Again, doctors have paid adult family members salaries for years. The extra cost of maintaining the corporation minimizes the small benefit. IF medical corporations were allowed to have trusts or other corporations as shareholders and were allowed to engage in other business activities, then yes, corps would be as big a benefit as they are in other provinces today.
As I said, incorporation benefits physicians IF, and primarily IF, they leave unspent income IN the corporation. The corporation serves as a tax deferred savings vehicle where funds may accumulate AFTER paying corporate taxes.
I suspect the example you offer compares a single income physician family with no income splitting and no incorporation to a fully income split, incorporated family. It’s like comparing a horse and buggy to a car when you should compare one car with another car.
I speak from personal experience on this. I have 4 children and my wife does not work outside the home. We struggle to leave income in the corporation as an alternative to RRSPs. While I’m incredibly grateful that we’ve been allowed to incorporate, it’s not the golden goose you portray it as, and the other provinces have allowed a more robust form of incorporation for years.
I appreciate you disclosing your government income. I would feel awkward asking for higher taxes to support my income source.
Cheers
Shawn
Hello Shawn. Thank you for your reply and your continuing dedication to presenting the physicians’ point of view. It is fascinating to see all the responses and feedback; this forum is a rare thing but clearly there is a need for it!
One question relates to your last comment. If I understand correctly, right now the OMA and physicians are especially opposed to numerous changes to how you are paid by the government, all of which are resulting in lower pay for physicians. Patient care, you are saying, will be affected by these cuts but it seems to me that the bottom line issue for you and the OMA is pay. But you also say that you would feel awkward asking for higher taxes to support your income stream. If that is the case, I guess I am confused, or maybe I have just missed part of the discussion. Could you tell me what is the physician proposal to fund the income stream at the level the OMA is asking for? If you are opposed to higher taxes, where do you propose the funds for maintaining your past level of funding come from? Thank you.
Thanks for gently pushing back, Tammy. It gives me a chance to respond. Much appreciated!
I’d encourage you to read the “Medical Fee Cuts and a Bakery” post. It explains, as clearly as I can manage, how fee cuts harm patients. Had the government been willing to discuss solutions to immediate care needs by discussing programs and innovation, I’m certain docs would have accepted ANOTHER large cut like they did in 2012. Because the current ‘take it or leave it’ offer decimated over a decade of improvements in patient care access, it would have been unconscionable to have accepted it. I repeat, I think docs would have taken another cut had government been willing to discuss solutions to immediate and pressing patient care needs.
You say, “…it seems to me that the bottom line issue for you and the OMA is pay.” If so, then why did the OMA offer to have their fees frozen (i.e., 0% increase) for 2 years? Zero percent doesn’t sound like a plea for more income to me.
Finally, you ask a fantastic question that I wish everyone in Ontario would ask. Where does the money come from? If we want a system that offers first-dollar coverage for everything it does today, and everything that will be invented tomorrow, how will we pay for it? Do we want more and more of the same? Do we want higher and higher taxes? If not, how have France, Germany, Britain, Sweden, Switzerland, and dozens of other advanced countries funded their healthcare systems? Please do NOT mention the USA. Everyone who wants to close debate immediately brings up the scary US system. I agree; the US system is scary. That’s why we should leave it out of the discussion.
Bottom line: government has the responsibility to fund care for the population. They’ve refused to fund growth in demand for medical care. They’ve balanced their books by slashing 12 years of improvements. It will harm patients.
Thanks again for your comments and questions!
Tammy please explain how much someone would have to save to age 55 to have a pension of 60,000 a year for the rest of their life like teachers. 13 years post secondary education. So how much per year after taxes has to put away from age 31 to 55 to be as well off as a teacher and don’t forget the 150,000 to 200,000 dollar debt to be paid off. Don’t get me wrong doctors are not starving but lifetime earnings of any professional in public sector is more than most doctors and most of our inflated earnings come from working 60 hours a week because there is no shortage of work just doctors.
Thank you, Shawn, for clearing that grave misconception and enlightening us to the reality of overtaxation! And bankruptcy, personal and government!
Cheers,
Donna
Thanks for commenting, Donna! Cheers, s
I would like to note that the comparisons to tradesmen (mechanics in the example above) is unfairly portrayed.
As a 26 year old who started my education path towards a medical career (completed undergrad in neuroscience) and who currently works in the trades this topic is of great interest.
At 115$ an hour they are also paying the same overhead fees you claim (owning or renting garage, licences, specialized tools, continuing education, office staff etc..) This is 115$ to pay the whole shop. A licensed mechanic working at a shop will make anywhere from 20-40$ (i’m not a mechanic these are numbers i’ve heard from some mechanics please correct me if i’m wrong). Another difference is you quote 33$ for fee per service which as you say can increase per hour, mechanics and tradesmen have to quote the job beforehand. Sometimes 3 billed hours took 5 hours in the shop.
I am not saying doctors should take paycuts, I believe they are underpaid for their effort and dedication (which is why I did not pursue that career). However the argument that trades are overpaid in comparison does not sit well with me.
Politicians are a whole different story.
P.s. apologies for typos etc, typed up quickly on my phone
To sum up my comment a little more elegantly…
I think Doctors are undervalued but wish to reduce the stigma of the “common tradesmen”
Thanks for both of your comments, Nathan! With a long history of working in trades and unions myself (both my brothers have been truck drivers over the years), I appreciate you jumping in. Thanks for clarifying shop fees. I realise that rounding up or down to the hour happens all the time. Your summary statement was brilliant!
Cheers,
Shawn
All the points you and Donna make in your original and follow-up threads are great and correct. However, as a HCP, I see lot of waste in healthcare, especially unnecessary imaging studies, that often lead to further unwarranted follow-up imaging studies.
Unnecessary Imaging in the past decade, is one of the major factors in increasing cost of healthcare and waste of millions of Dollars. Unfortunately, neither OMA, nor the Government is talking about this issue.
If we could discuss this imaging issue and work on this then it likely would be win-win situation for both parties. Government likely wouldn’t talk about this because they may loose votes in future elections. Government wouldn’t make a Rational decision, and often they survive and proliferate with irrational decisions, but we as HCP need to do something about this waste!!!, And SHARE the PIE Better.
Great point, Loveleen! Patients often want investigation, radiologists recommend additional studies, and primary care docs order tests to protect themselves medicolegally.
A number of system savings work groups spent the summer on these things in 2012. In fact, $850 million savings were found in 2012-2014 by the government’s own estimation. But we need to do more.
I agree we need to use the pie we have better. We also need to discuss how big society wants the pie and how to make it fit society’s expectations.
Thanks again!
Shawn
You’re absolutely correct, Loveleen! Thanks for bringing that up and Shawn for reinforcing the savings already made, but more needs to be done both in radiology and other labs! I can’t tell you how many people ask for their cholesterol to be retested, even though they haven’t changed their diet!!!
It’s so incredibly time consuming to educate patients about the overuse and needless waste.
Here’s a really bad scenario. And where I feel that there should be some reigning-in of this practice: docs who are ordering “hormone tests” on women in the peri-menopuause/menopause years…..WHAT A GLARING BLATANT WASTE! Last week a rostered patient of mine went to a naturopath regarding her chronic fatigue and “had a bunch of tests that she said were all normal”. I asked the patient if she paid out of pocket for these tests. She replied that she hadn’t, that the naturopath works with a general practitioner who orders the bloodtests….site-unseen! THAT really gets my goat!! AND last year I came across a huge battery of tests ordered by a physician on a patient of mine, a 60 year old woman with no period for 5 years, and he had ordered estrogen and FSH and too many other needless hormone tests! What was he expecting to find?? OF COURSE her tests would be consistent with frank menopause! What happened to clinical acumen?
I have called the CPSO about this, and I didn’t get past the receptionist who told me simply, “the public of Ontario is allowed to seek whatever kind of medical care they want”. That’s the great physician support we get in our province.
Anyway, once again I am reduced to ranting.
That’s enough!
Many thanks to all, especially Shawn for his intuitive letters, backed by excellent knowledge and research! You are awesome and inspiring,
Donna
Wow, loads of passion from personal experience in that comment, Donna! I love it.
Of course, you make a solid point. Whenever I see my colleagues doing something I think is totally crazy, I wonder what I’m missing. Was there some other reason for ordering the tests? Was there a simple mistake? What went through the doc’s head at the time? I wonder whether something that appears so clearly off in hindsight must have included something we don’t see.
The comments have definitely turned out to be the highlight of these posts, by far! Thanks so much for helping to make this conversation so much better than it would have been without your participation.
Much appreciated!
Shawn
You are so right. A lot of waste govt needs govern and manage this
Hi Shawn:
Thanks for the blog and all the response generated.
I have 2 comments I thought you and your readers might find at least thought-provoking.
#1) Salary-I am a salaried physician. Less than 5% of all doctors are on a true salary (I can’t post the source, but I know it’s out there somewhere). I have only been a family doctor for 8 years. I have worked on contract, then pure FFS, then as a salaried physician. I have worked in 2 provinces. I have never been happier than I am now. I have 6 children so trust me I literally *need* to make money. I once read another MD blog that posed the question, “Do you feel like an assembly line worker?” That was so true while I worked FFS. What I lose in pay I gain in benefits: Full medical, dental, life insurances all paid, top-rated HOOP pension, and NO overhead or dreaded tax installment headaches. I have never been happier. My own doctor tells me I’m lazy and should be hating this work–secretly she confided in me at my last visit that she was jealous! Just sayin—-there is the salaried option, it’s just so rare for MDs to pursue it.
#2) MSP Blue Book–Google it–Every single physician’s billings are listed there by provincial law. It’s often a source of embarrassment, greed and chuckles when it comes out every year. This is for the province of BC. One of your readers did point out that many a GP can make a lot of money–This is so shockingly true (but I think a minority) when you read something like the Blue Book. In a small town in BC I know of 3 GPs who billed more than an orthopedic surgeon or plastic surgeon. However, I must say that patient care suffered from these guys tactics (or so was the perception). They worked shockingly hard and fast–the kind of medicine style I said I NEVER wanted to practice.
Food for thought.
Great comments, Ken! Thanks so much for taking time to share them. I didn’t know about the MSP Blue Book. I will try to find it.
Many share your comments about salary. I think politicians know that there’s no way they could afford to run Medicare without a good chunk of physicians willing to run like hamsters. It usually takes 2.5 salaried workers to perform the work of 1 FFS employee. Government knows this.
Thanks again for sharing your thoughts!!
Shawn
Just a bit more perspective for some of us practising.
I trained abroad…I chose to do so, when I couldn’t get a spot in Ontario, but still really wanted to be a physician. So, I went to England.
I paid $200K in tuition
I came in the top 5% of my class.
Then I paid thousands to come back.
I chose to do that too.
But where I work currently, I am filling a hugely needed physician void.
I qualified for $10,000 OSAP roughly in the 4 years I was away.
I now pay > 2 mortgages paying back my student loans.
This was, to me, reasonable, to do what I love where I love to live.
Now there are cuts.
I am wondering how we will squeeze through one more month just barely paying off my tuition fees and taxes.
We are now selling our house, as the cuts start.
Grim
Oh Jessica, what a painful note! Perhaps the way you wrote it, with spaces between short statements, but for whatever reason, it really moved me. Even for those of us who love the work, it becomes a business decision. We cannot stay in practice when the margin between expenses and income becomes too small. I have had to sell the first new vehicle I have bought, ever. I worry I won’t be able to make payments. With EMR funding ending, forced pension payments, increased overhead and cuts on top of that, I cannot make it following my romantic dream of a small rural practice without some significant sacrifice.
I’ll see how the next few months go for me. I’m already looking for other options to supplement income for my family.
Yikes, I’m sharing too much…
Thanks YOU for sharing this note. I know you will find a spot that truly values the invaluable skills and service you offer patients.
Hoping the best for you!
Shawn
Hi Shawn and Jessica,
It is very grim. I know you’ve seen all the FB banter, and about 1/3 of us are up in arms. What can we do, I’m in the same boat. I have had to pay out of pocket for 2 EMR’s, the first bankrupted just as I was getting quick with it, and then 2nd I’ve been battling to learn for over a year now. Such frustration, and at 57, I don’t think I can tolerate another financial hit. It’s too expensive to afford all the staff and overhead I have right now, so any further decrease is going to affect me badly. The fight is supposed to be about cuts affecting care, and ultimately anything further will be disastrous, but for me personally, it is about the money.
Good luck to you both, and to all the doctors in Ontario who are worrying about their future and the future of healthcare.
Donna Mahoney
Thanks Donna! I think many more doctors are thinking this than not. Even IF the average MD billing used to be $360k in Ontario before overhead, the average for family practice was much lower. That means many thousands of us are earning in the mid to low $100k after overhead. That still sounds like a lot, but it compares with a salaried position of around $100k. Our NPs make just under $100k and have only 500-800 hours of training after nursing. We have 10,000 hours after our first degree.
Overhead isn’t just a cost; it’s a responsibility. A fridge costs money. Hiring staff requires time, energy and management, not just money.
For those of us trying to work part-time at family practice, it will require some significant changes. We will need to drastically trim down the services we offer just to save overhead.
Thanks again for writing! It helps to know others are feeling the same.
Warm regards,
Shawn
Hi Shawn and all the doctors who posted comments on this website.
Not sure if I’m allowed to add my thoughts to these comments but I’m going to try. I have an amazing doctor for 18 years now. He works 7 days a week and during those 7 days has 3 walk-in clinics for his patients only. He is running like a hamster on a wheel and its very hard to get a regular appointment with him, which is why he has walk-ins. However if you’re not lined up at 7:30 a.m. for his walk-in that starts at 8:00 a.m you will be waiting until lunch time to see him. Because of this, I occasionally go to one specific walk-in clinic and usually see the same doctor. To make a long story short, I broke my foot on Saturday/Halloween. I didn’t bother going to the hospital because I didn’t want to spend the rest of my weekend in the waiting room as this has happened before, so I had a walking cast,strapped it up and called my family doctor on Monday to see if I could make an appointment. I was told by his assistant that they were booked all day Monday and Tuesday. So, I went to the walk in clinic as I wanted to know if my foot was broken for real, or if it was just a sprain as I had to go to work. After my Monday morning visit with the walk-in clinic doctor, my family doctor called me and told me he wanted to see me as a follow up, I had him copied on my Xray results, so I went in at 7:30 a.m. Friday morning and was scolded by him for going to the walk-in. He told me he only makes $60 dollars a year for having me as a patient (I’m 53 and things are starting to go wrong) and that my visit to the walk in cost him $30. I listened to what he had to say, fuming inside mind you, and then came home and started searching websites to see if there was any truth to what he was saying. Low and behold I found this website and now I know where he’s coming from. I want to apologize to him for what I was thinking, ie: it’s all about the money for him, but its next to impossible to talk to him or send him an email. I totally agree with a past post that the fee information should definitely be posted for the patients review. It would help patients understand where doctors are coming from.
Thank you and I hope you post this comment.
Thank you, Donna, for sharing your story!
I am so sorry to hear what you went through. I sure hope your foot improved, and you’re back doing the things you enjoy.
I only wish I could tell you all the crazy incentives in our system that drive us. They make the patient experience unpleasant and confusing, if not unsafe at times. We need to advocate for a system that aligns incentives around patients. Doctors, nurses and hospitals should be rewarded when they meet your needs with high quality service as efficiently as possible. Right now, doctors get rewarded for more visits, hospitals get punished for more visits and nurses work to limit visits because visits just mean they have to work harder for the same income. It’s chaos.
Thank you so much for sharing your note! If more patients get informed and start asking for aligned incentives, we might see some positive change.
Kind regards,
Shawn
As a family doctor in Ontario; we are still doing FAR better than we did even 10 years ago. Our compensation is on par with our American counterparts now and the average family doctor is taking home OVER 200k after overhead. With the cuts, we will still be over 200k. Please stop the whining.
Thanks for sharing your comment!
No question, doctors who work hard, train for 20 years or so, then continue to work hard will earn a very decent income. But that’s not the point, is it? Cuts to spending on medical services decrease the amount of services available for patients.
I hope you do not tell new graduates to ‘stop whining’. Pretty heartless when the banks are foreclosing on their student loans after Wynne cut their first year net earnings by 40% (yes, forty percent).
Thanks for taking time to write.
Shawn
Shawn
I glad to know about this information that you mentioned above.I need this information.It is useful to me.I am waiting to get more information from your site.
Thanks for sharing this information to all..