
Who wants average healthcare? We want the best for our children and loved ones, not average. Canadian Medicare can never deliver excellence, because it’s made to deliver equality.
Excellence does not occur by chance. We design systems to produce and reward excellence. But, Medicare hates reward based on performance.
Medicare delivers equal pay and equal performance, but not excellence.
Most big healthcare organizations are unionized in Canada. Unions discriminate on seniority; the longer you work, the more you make. Volume or quality of work does not change unionized income or job status.
But, we DO discriminate by punishing the very lowest performers. Gross negligence will get you fired, or sent for remedial training.
So, more accurately, Medicare just refuses to reward excellence. In fact, Medicare finds distasteful the idea that some perform better than average.
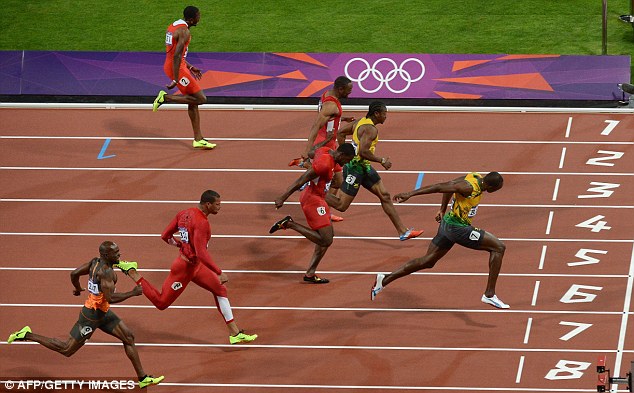 Every Olympic race has a few speedy people out in front, a pack in the middle, and a few of the slowest at the end. Medicare denies that bell curves exist; that there’s any race at all.
Every Olympic race has a few speedy people out in front, a pack in the middle, and a few of the slowest at the end. Medicare denies that bell curves exist; that there’s any race at all.
Excellence requires effort, exposure, and risk. Why reach for excellence to earn weak kudos from your boss and disdain from colleagues for making them look bad? Inspiring leaders can squeeze out extra effort, but always backed by the promise of rewards: better pay, better positions, or better intangible benefits.
When we remove the concept of excellence, all measures of excellence, and refuse to reward excellence, we leave nothing for management to lever. All that’s left is process and structure. Management defines work that needs to be done and relies on punishment if it’s not done. Punishment invites union scrutiny. Performance management gets tried, found difficult, and left undone.
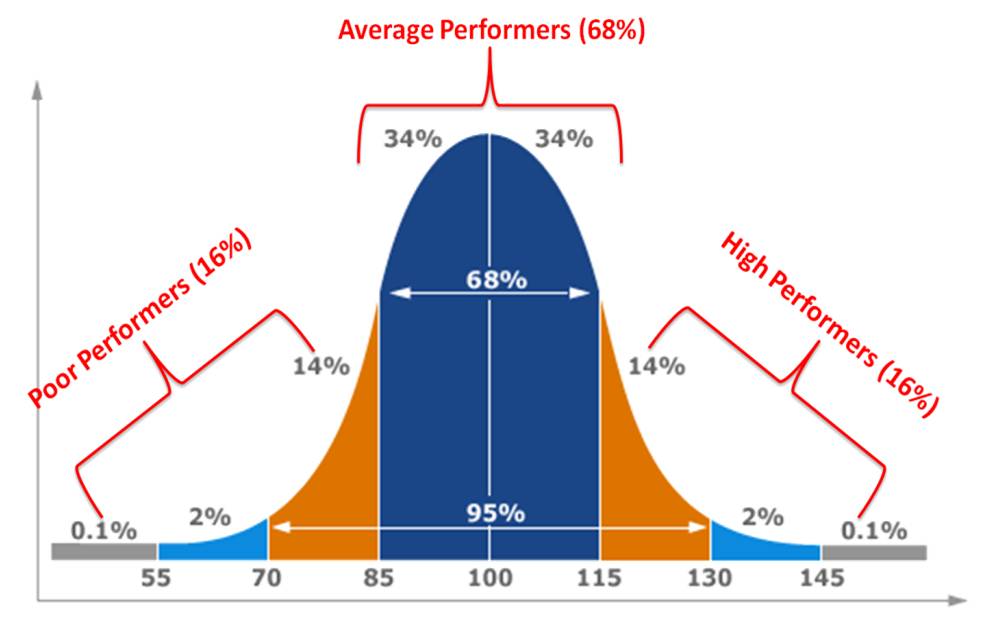
Refusal to reward excellence drives revision to the mean. Everyone clusters around the average; the bell curve becomes narrow and steep…equal and safe.
When everyone’s performance is average, patients get average care. Unless we have unlimited budgets, excellence can never show up, except by chance or revolution.
Do we care about excellent patient care, or provider equality? In times of fiscal restraint, ideologic commitment to equality cheats patients of excellence by offering only average healthcare.
(photo credit: blog.ubc.ca)

